AN OVERVIEW OF CHRONIC CANDIDIASIS
One of the challenges that the human race faces today is the pandemic fungal infection known as Candida, also known as Systematic Candidiasis. Systemic means “in all the body”.
Many practitioners of allopathic as well as natural medicine have tried to treat Candida with varying success. In order to understand the treatment, one must understand how Candida behaves within its life cycle.
Studies have shown that 90% of newborn babies have the normal, budding Candida in the gut. This is a unicellular cell that reproduces asexually producing a daughter cell. It is non-pathogenic and sits in the gut without producing symptoms and belongs to the vegetable kingdom.
Like their “cousins” the moulds, they live all around you. One large family of yeasts is Candida albicans, with over 81 different species – they live harmoniously in the mouth, throat, intestines and genito-urinary tract of most humans, and is usually considered to be a normal part of the bowel flora.
C. albicans is a diploid organism which has eight sets of chromosome pairs. Candida is one of the few microorganisms that has a diploid gene controlling the same protein- this means that it is capable of pleomorphic activity, being able to mutate from the budding form to the mycelia (fungal), pathogenic form.
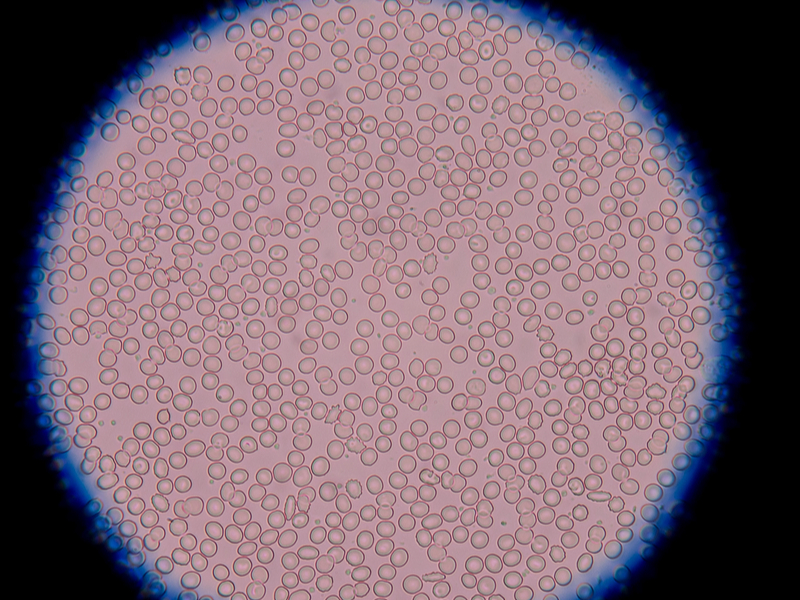
The problem begins when the normal (image left), budding candida species that we all have in our gut undergoes pleomorphic changes and begins forming mycelial or hyphae forms – this form of Candida is pathogenic and can cause a large myriad of symptoms.
This happens when the internal milieu of the gut and other tissues become more acidic, therefore killing off many of the friendly bacteria of the Acidophilus and Bifida species. This can occur either through taking a variety of drugs such as antibiotics, cortisone, anti-inflammatories and chemotherapy used for cancer cases – the bowel flora can also drastically reduce when the pH of the body becomes too acidic – eating sugar and other refined products in large quantities can create this acidity.
It appears that this change in pH can trigger genes in the Candida to begin a pleomorphic change into a stealth organism that is very active – if fed with sugar, it can increase itself from 1 to 100 cells in 24 hours. These 100 cells can then produce 100 each in the next 24 hours, and so on. And so by the 4th day we will have 100 million Candida cells.
Most practitioners trying to treat Canidida will concentrate on killing off the pathogenic, mycelial form, without addressing the significant question of converting this pleomorphic form back to the normal, budding form using the Sanum remedies. Another reason for the large numbers of failures by health practitioners is that the internal milieu is not addressed, and also the diet, which is crucial. We will come back to these important points when we discuss treatment protocols.
THE PARASITIC ROLE OF CANDIDA
Candida has two parasitic functions:
1. It gobbles up any putrefied food matter in our digestive system (mostly caused by improper digestion due to low stomach acid).
2. After we die, Candida acts to decompose the body by secreting phospholipid enzymes, feeding off our corpse and returning us to Mother Earth. When conditions are right, it transforms itself from the “bud” state into the mycelial state, where filament-like roots invade deep into the mucosa in search of nourishment.
The mycelia release phospholipase, an enzyme that attacks cell membranes of the mucosa, splitting fatty acids, generating free radicals, and causing inflammation in the intestine.
Wherever the yeast colonise they cause symptoms, whether an itchy anus or vagina, diarrhoea, heartburn or sore throat. The mycelial forms release 79 different toxic by-products that damage specific tissues and organs and will determine which symptoms will occur. These mycotoxins can also compete with hormone receptor sites, causing hypothyroidism, hypoestrogenism, as well as binding cortisone, progesterone and other hormones for its own use and causing endocrine deficiency states.
BRIEF HISTORY OF CANDIDA
Hippocrates describes oral candidiasis (around 400 B.C.) as “mouths affected with aphthous ulcerations”. In 1665, Pepys Diary reported “a patient hath a fever, a thrush and a hiccup”, immortalize the idea that oral thrush establish from the host.
In 1771, Rosen von Rosenstein defined an invasive form of thrush.
In 1839, Langenbeck was credited with first recognizing a fungus in a patient with typhoid fever. He describes in detail what is now referred to as septate hyphae, branched pseudohyphae and blastoconidia. However, he recognized the entity to the typhoid bacterium rather than the fungus.
In 1847, French mycologist, Charles Philippe Robin, classified the fungus as Oidium albicans using Albicans to name the fungus causing thrush.
Christine Berkhout and others observed the ability of this fungus to infect humans. Berkhout reclassified it under the current genus Candida, in 1923. Berkhout’s taxonomy was later made known by the French mycologist, Maurice Langeron and Paul Guerra as “the beginning of the rational systematics of the non- ascosporogenous yeasts”.
OTHER FACTORS CREATING PATHOGENESIS
The pathogenesis of disease associated with Candida in humans is driven by a multitude of factors. Some strains of Candida produce gliotoxin, which may impair neutrophil function. However, Candida is a polyantigenic organism containing up to 178 different antigens, which might explain the number of cross-reactions to yeasts, moulds and even human tissue.
It was shown recently that there is a potential cross reactivity with gluten because of several amino acid sequences that are highly homologous to alpha-gliadin and gamma-gliadin. Such a mechanism might lead to wheat intolerance with its accompanying symptoms, and even trigger Coeliac disease in genetically susceptible people. Furthermore, a placebo-controlled crossover study has revealed that dietary yeast may affect the activity of Crohn’s disease.
Candida produces alcohol and contains glycoproteins, which have the potential to stimulate mast cells to release histamine, and apparently prostaglandin-inflammatory substances that could cause IBS-like symptoms.
MYCOTOXINS
Toxic waste from mycotoxins from Candida infestations can also be absorbed into the bloodstream causing “yeast toxin hypersensitivity”, leading to many symptoms such as anxiety, depression and impaired intellectual functioning.
The main toxin implicated here is acetaldehyde, which is a normal by-product of metabolism, produced in small amounts and rendered harmless by the liver. If however, there is excess production of this by Candida, particularly in low-oxygen environments, and a lack of the appropriate liver enzymes – which tend to be deficient in 5 per cent of the general population – the acetaldehyde will become bound strongly to human tissue. This may cause impaired neuro-transmission in the brain, resulting in anxiety, depression, defective memory and cloudy thinking.
Some 40 – 60% of all immune cells in our body are in the gut. The immune system may also concurrently be adversely affected by poor nutrition, heavy exposure to moulds in the air, as well as an increasing number of chemicals in our food, water and air, including: petrochemicals, formaldehyde, perfumes, cleaning fluids, insecticides, tobacco and other indoor and outdoor pollutants.
Exclusively, yeasts tend to secrete a toxin called gliotoxin, which can disrupt the immune system by inactivating enzyme systems and producing free radicals, thus interfering with the DNA of leukocytes.
The resulting lowered resistance may not only cause an overall sense of ill health, but may also allow for the development of respiratory, digestive and other systemic symptoms. One may also become predisposed to developing sensitivities to foods and chemicals in the environment.
Heavy metals such as mercury and others are found in higher amounts when Candida is present, as the Candida yeasts actually store the metals in their cells – these metals are then released when the Candida die during treatment. This is why it is important to undergo a natural, heavy metals detox while treating Systemic Candidiasis.
Candida is sensitive to a number of antifungal agents, such as Nystatin, which is not absorbed from the gastrointestinal tract after oral administration. It destroys Candida by binding to sterols in the cell membrane, and thereby increasing permeability with loss of cellular contents.
When other health conditions become involved, Candida becomes known as Candida-related complex (CRC). CRC, an excess of Candida in your system can cause a host of uncomfortable signs and symptoms which are syndromes within themselves, such as chronic fatigue syndrome, hypoglycaemia, leaky gut syndrome, fibromyalgia, allergy or sensitivity, hormonal, thyroid, and adrenal dysfunction.
This syndrome isn’t caused by Candida itself present in our mucosal tissues that cause irritation, inflammation, itchiness, redness and pain but by the amount of metabolites from the yeast colonies released inside the human colon when they exceed tolerable amounts.
Patients with CRC often have widespread symptoms affecting multiple organs systems such as:
- Gastrointestinal symptoms
- Chronic allergies
- Unexplained fatigue, always tired
- CNS fog, mood swings, depression
- Skin rashes, fungal infections
- Cravings for sugar, bread, beer
Toxicity in the colon affects the health of the whole body particularly if one’s elimination is slowed as in the case of constipation due to an imbalance in intestinal flora.
The delicate hormonal and chemical balance that orchestrates our emotional health can also be affected causing symptoms of mental illness.
EVERYONE CAN BE AFFECTED WITH CANDIDA!
Anyone can be infected with Candida today! Women can be infected because of antibiotics, steroids, anti-inflammatory medications, hormones and birth-control pills. Men are also being infected with Candida from antibiotics, steroids, anti-inflammatory drugs, pain medications, and sexual relations with an infected partner, even though this often results in a topical infection, not a systemic spread.
Teenagers get Candida from routine treatment with tetracycline or other antibiotics for acne. Babies have Candida from the birth canal or breast milk of the infected mother. That is why babies often have thrush (a white- coated tongue), which is a yeast infection.
Millions of people all over the world are infected with Candida. It is estimated that at least one out of three people in the Western world are affected. Because so many of the population can be infected and because so many factors can cause the condition, Candida is an enormous health problem today and has truly reached pandemic proportions.
Candida coexists in our bodies with many species of bacteria in a competitive balance. Other bacteria act in part to keep Candida growth in check in our body ecology. When health is present, the immune system keeps Candida proliferation under control, but when the immune response is weakened, Candida growth can proceed unchecked. It is an opportunistic organism, one which, when given the opportunity, will attempt to colonize all acidic bodily tissues – this is one of the reasons why it is present in all cancerous tumours as they have a very acidic pH. This uncontrolled growth of Candida is known as “Candida overgrowth” or “Candidiasis”.
UPSETTING THE ECOLOGICAL BALANCE OF THE BODY
Unfortunately, there are many factors in our modern society that can upset the ecological balance of the body, weaken the immune system and thus allow the yeast to overgrow.
The major risks factors are:
- Steroid hormones, immunosuppressant drugs such as cortisone, which treat severe allergic problems by paralyzing the immune system’s ability to react.
- Pregnancy and birth control bills which upset the body’s hormonal balance
- Diets high in carbohydrate and sugar intake, yeast and yeast products, fermented foods
- Prolonged exposure to environmental moulds
- Antibiotics and sulpha drugs – probably the chief perpetrator of all-antibiotics that kill ALL bacteria, good and bad. They do not distinguish good bacteria from bad. Antibiotics kill the “good” flora which normally keeps the candida under control. This allows for the unchecked growth of candida in the intestinal tract. It is normally difficult to recover a yeast culture from bodily surfaces.
In a variety of ways the same thing happens with the use of steroid drugs, such as cortisone. All steroids, including the contraceptive pill, will have a depressing effect on the immune system, as well as killing off friendly bacteria in the body.
Yeast infections are common in those that take repeated or prolonged courses of amoxicillin, ampicillin, ceclor, keflex, tetracycline or other broad- spectrum antibiotics during infancy, childhood, adolescence, or since you are become an adult.
DIETARY FACTORS
Sugar is the main nutrient of Candida albicans. Candida albicans thrive on all simple sugars, sweeteners, but also natural sugars in fruits and fruit juices, as well as eating too many complex carbohydrates.
There are several reasons to restrict or eliminate the intake of milk in patients with chronic candidiasis:
- High lactose content promotes the overgrowth of Candida
- Milk is one of the most frequent food allergens
- Milk may contain trace elements of antibiotics, which can further disrupt the gastrointestinal bacterial flora and promote Candida overgrowth
DO YOU HAVE CANDIDA? HOW DO YOU KNOW YOU HAVE IT?
The patient’s history and symptoms is usually the key to arriving at a diagnosis. There are a wide variety of signs and symptoms that are prevalent in systemic Candidiasis, being able to score these systematically provides a good, overall picture. Dr. Crook’s Candida questionnaire is very helpful as it enables the patient to score their symptoms and arrive at a number, anything above 180 for women, and 140 for men is highly significant and represents the majority of symptoms that relate to the Candida.
There are also other testing procedures for diagnosing Candida, using VRT Bioresonance diagnostics such as VEGA Biodermal screening. Using this technology, the practitioner is trying to determine if there is a resonance response with the patient, using an ampoule of pathogenic Candida. If there is no pathogenic Candida in the patient, then there will be no resonant effect, and this is easy to measure using this equipment.
Another method of testing the Candida is to use a form of kinesiological muscle testing called Autonomic Response Testing (ART) invented by a German neurologist Dr. Dietrich Klinghardt, M.D. Ph.D. ART grew out of the importance of detecting and correct problems of the autonomic nervous system (ANS).
ART allows the practitioner to correct the problems of the ANS and to help restore the self regulating mechanism of the body allowing the patient to return to a state of health.
To date, there is no conclusive blood or clinical test for diagnosing pathogenic Systemic Candidiasis. In time to come there will probably be genetic tests that can determine the genome of the mycelial, pathogenic Candida.
Let us now examine the concept of treatment which is quite complex if one really wants to succeed. There are numerous approaches to treating Candida which are used; from medical doctors using medicinal anti-fungals to naturopaths and nutritionists using a variety of natural products to kill off the Candida. All these treatments are rampant with problems that end up in the patient feeling better initially, only to find that the Candida “creeps back” again after a few months.
Dr George John Georgiou, the author of this paper and an internationally renowned Holistic Medicine Practitioner had researched and experimented, treating his own Candida for many years. He spent many years visiting many medical and natural medicine practitioners, but found that no-one was able to treat his Candida successfully and fully. Eventually, after 11 years of trial and error, he managed to put together a protocol that goes further than traditional schools – he has used this treatment protocol for over 10 years now and has successfully treated in excess of 3,500 patients to date.
As this treatment protocol is being implemented at the Da Vinci Holistic Health Center, Larnaca, Cyprus where Dr Georgiou is the Director Founder, it has come to be called the “Da Vinci Candida Treatment Protocol”. Dr. Georgiou now treats patients from all over the world and one of his nicknames is “Dr Candida.”
THE DA VINCI CANDIDA TREATMENT PROTOCOL
There are toxins in the food you eat, the water you drink and the air you breathe. Even your own body produces toxins as a result of its many metabolic processes that keep you alive.
Before implementing the Candida Treatment with patients, Dr Georgiou therefore makes certain that the patient goes through a detoxification protocol to balance the internal milieu. One of the quickest, cheapest and most efficient ways of achieving this is to undergo a 15-day alkaline detox programme using only fresh fruits, vegetables, vegetable juices and soups, steamed vegetables with olive oil and herbs, as well as herbal teas.
There are a number of benefits of detoxification such as:
- The digestive tract is cleansed of accumulated waste and fermenting bacteria.
- Liver, kidney and blood purification can take place, which is not possible during regular eating patterns.
- Mental clarity is enhanced as chemical and food additive overload is reduced.
- Reduced dependency on habit forming substances such as sugar, caffeine, nicotine, alcohol and drugs,
- The stomach size is returned to normal as bad eating habits can be stopped.
- The hormonal system is enhanced which is especially true for growth hormones.
- The immune system is stimulated.
After detoxifying on an alkaline diet for 15 days, patients report higher energy levels, clear and glowing skin, weight loss of several pounds, clear-headedness, reduced cellulite, good body tone and a great feeling of being relaxed.
THE DA VINCI CENTRE DETOXIFICATION DIET
We suggest that the person eat only fresh fruit, salads, freshly squeezed juices, steamed vegetables and vegetable soups for 15 consecutive days.
These are the foods that are allowed during the detoxification phase, no other family of foods is allowed. You may eat as many of the following foods as you wish, but it is best to eat only when you feel hungry. Wash all fruit and vegetables in a bowl of water with 4-5 tablespoons of grape vinegar added to help wash away any pesticide/ herbicide residues. Rinse afterwards with clean water. Here are the foods that you can eat in plenty:
Salads – use any type of fresh vegetables you like, in any combination. Use organic vegetables when available, and include bean sprouts when in season. Salad dressings should be kept simple- a little virgin olive oil with fresh lemon, or cider vinegar. Add plenty of fresh onion and garlic- these are very detoxifying.
Steamed vegetables – eat any variety you like, including broccoli, cauliflower, potatoes, beetroot, carrots etc. Steam as opposed to boil, and eat with a little herbal salt, lemon and a little virgin olive oil, with plenty of garlic.
Vegetable/fruit juices – drink a minimum of 1-3 per day, and try to include one cocktail comprising one- third of a glass of raw green juice (spinach, parsley, cabbage and any other green vegetables), topped up with carrot juice. Carrot juice has a strong effect on the digestive system, provides energy, serves as an important source of minerals, promotes normal elimination, has diuretic properties and helps to build healthy tissue, skin and teeth.
Fresh Fruit – choose the fruit of your choice and eat as much as you like, whenever you like. You could begin the day with 2-3 pieces of fruit, which are gentle on the digestive system. Make a tasty fruit salad. Try to avoid too many juicy fruits as this may overly feed the Candida, and certainly avoid all forms of fruit juices as this will give sugar to the body quickly, again feeding the Candida. There is tremendous benefit in adding fruit during the detox due to their living enzymes and phytonutrients which are very cleansing to the body. Remember, we are not treating the Candida yet, only helping the body to cleanse and prepare for the 3-month Candida protocol.
Herbal teas – choice any of your choice. Chamomile is a good relaxant, aniseed and mint is good for the digestive system, Kombucha, dandelion tea which is excellent for purifying the blood and detoxifying and stimulating liver function, sage tea which is a blood cleanser, nettle tea which is excellent for driving away excess fluid out of the tissues and is a wonderful cleanser for all the detoxification organs. Drink as many as you like, with a little honey on the tip of a teaspoon if you like.
The purpose of this diet is to detoxify – to remove the toxins from the fat cells and tissues as well as the organs, so that the body can return to its optimum level of functionally.
PARASITES, HEAVY METALS AND OTHER TOXINS
As part of the detoxification process, the Da Vinci Center also attempts to detoxify heavy metals that can easily be detected using a hair analysis sent to a US laboratory of repute.
In addition, there are also parasites which more than 90% of people carry, so it is good to also incorporate a parasite cleanse in with the 15-day detox diet.
Heavy metals are found from fish and amalgam fillings (mercury): aluminium found in cheeses, baking powders, cake mixes, self- raising flour, cosmetics, toothpastes, antiperspirants and some drugs such as antacids.
Arsenic is given to chickens as a growth-promoter, cadmium is found in tea and coffee, as well as cigarette smokers. Lead is found in paints, fuels, rubber, plastics, inks, dyes, toys, building materials and hair restorers.
One of the most researched natural chelators in the world that has undergone double-blind, placebo controlled trials with 350 people is called HMD™. It has been shown to safely chelate many different types of heavy metals, including uranium, a difficult metal to chelate.
As part of a novel approach to eradicating parasites, the use of small, portable bioresonance devices invented by Russian scientists called Deta Elis have been used with good success.
Let us now examine the Da Vinci Candida Treatment Protocol in more depth.
The Da Vinci Candida Protocol has five basic objectives:
- Starve the Candida by eliminating the foods that feed it
- Kill the Candida through the use of anti-Candida natural products
- Repopulate bowel flora with a high-potency probiotics such as Custom Probiotics, an excellent American company that specializes only in probiotics – the capsules are guaranteed to contain 60 billion live bacteria one year after manufacture.
- Regulate the dysbiosis and convert the pathological, mycelia form of Candida back to the normal form by the use of the Sanum remedies produced by the Sanum Kehlbeck company in Germany.
- Restore biochemical balance to the body and strength to the immune system. This will allow the body once again to regain and maintain control over Candida growth by optimizing the diet – this would involve avoiding food intolerances and following the Metabolic Type diet by Bill Wolcott. Also kill off parasites and chelate heavy metals out of the system.
Let us examine these steps in a little more details below:
Phase 1 – Starving the Candida
The foods that should be strictly AVOIDED during that time include:
- Sugar– and all foods that contain sugar. These include white and brown sugar, honey, syrups, liquor, lactose, fructose, all confectionary and sweet cakes, chocolates, ice-creams, home- made sweets and cakes, biscuits, fizzy beverages and all fruit drinks.
- Yeasts – and all foods that contain yeast including breads, vinegar, ketchups, mayonnaise and pickles.
- Mushrooms– all types, including Chinese mushrooms such as Shitake
- Refined foods– all white flours, white rice, white pasta products, corn flour, custard and refined cereal products, unless they are whole meal or organic.
- Fermented products – all alcoholic beverages, vinegar and all vinegar products such as ketchup, mayonnaise and pickles, beer.
- Nuts – all types of nuts that are cleaned and packaged without their shells- these have a tendency to collect fungal spores and moulds from the atmosphere, which will antagonize the Candida. Nuts that are fresh with their shells are OK.
- Fresh and dried fruit – all fresh fruit should be avoided for the six weeks only as again, the fructose they contain will feed the Candida and make it extremely difficult to eliminate.
All other fruit that is not fresh such as cooked, tinned or dried and fruit juices should be avoided for the full 3 months.
Phase 2 – Killing the Candida
There are a number of herbal formulas, homoeopathic, isopathic remedies (Sanum) and probiotics that are used in the Da Vinci Candida Protocol – they have been carefully selected after years of experimentation, and the fact that they have worked time and time again with hundreds of people. The aim of using these supplements is to kill off the Candida.
Here are the supplements in order
- Kandidaplex– a doctor- formulated compound that contains Berberine, undecylenic acid, biotin, Sorbic acid, Pau D’ Arco and resveratrol from Japanese knotweed (Polygonum cuspidatum) root extract.
KandidaPlex™ features calcium undecylenate, a fatty acid that helps the body balance colonization of Candida. This formula also includes natural ingredients such as pau d’arco, berberine, and a vegetarian enzyme blend, formulated specifically to balance the growth of Candida albicans and improve the intestinal microenvironment.*Dosage: 2 capsules x 3 daily
- Horopito – a New Zealand herbal product that contains two powerful anti- fungal agents that have been shown to kill Candida- Pseudowinterata Colorata and the synergistic herb aniseed, that boosts effectiveness 6 fold. This herb has undergone scientific research and it has been found to be as effective as Nysteral and other anti-fungal medications, but without the side effects. Dosage: 1 capsule twice daily
- Caprylic acid (600 mg) – a derivative of coconut that stops the Candida reproducing, as well as killing the Candida.Dosage: 1 tablet x 3 daily
- Candida 30c homoeopathic nosode made from pathogenic Candida to kill off the Candida homeopathically.Dosage: 2 pillules x 3 daily for 2 weeks only. These are stopped just as the Sanum remedies are begun.
Phase 3 – Repopulating the Friendly Bacteria
This phase runs parallel with phase 2 and uses good quality, human strain probiotics such as the high-potency Custom Probiotics containing five superior strains of freeze-dried probiotic microorganisms that specifically target and help the small and large intestines, improving the intestinal microflora and digestive processes. These are:
• L. Acidophilus
• L. Rhamnosus
• L. Plantarum
• B. Lactis
• B. Bifidum
At the time of manufacture, each capsule actually contains 96 billion live bacteria, but are guaranteed to have a minimum of 60 billion one year later. They are also resistant to higher temperatures for a short period of time, making them convenient for travel for small periods of 2-3 weeks. Dosage: 1 capsule x 3 daily
To these supplements we add a good- quality multivitamin such as HMD MULTIS (2 caps x 2 daily) as well as Omega 3,6,9 fatty acids (1 caps x 2 daily) to provide all the vitamins and minerals that the immune system requires for optimal functioning.
Phase 4 – Using Isopathic Remedies to Normalize Pathogenic Candida
All the above must be taken for the full 3 calendar months of the protocol, with the exception of the homeopathic Candida 30c. After two weeks of the anti-Candida diet, certain specialized isopathic remedies are introduced, known as Sanum remedies from Germany, after the work of Prof. Enderlein, the father of pleomorphism and live blood analysis. Each of these isopathic remedies is only taken a couple of times per week, as follows – see also table below:
Mucokehl D5 tabs – 1 tab, twice weekly
Pefrakehl D4 caps – 1 cap twice weekly
Notakehl D5 tabs – 1 tab twice weekly
Nigersan D5 tabs – 1 tab twice weekly
Albicansan D4 caps – 1 cap every second day

Table showing schedule for taking Sanum remedies
If there is vaginal discharge, or anal Candida, then vaginal or anal pessaries of Albicansan D3 must also be used to eliminate this topical infection. These can be used every second day last thing at night, after sex.
These Sanum remedies mentioned above are continued for 10 weeks until the end of the Candida protocol. It is wise to begin the Sanum remedies TWO WEEKS after beginning the general protocol in order to allow a considerable portion of the Candida to die off, and to reduce the severity of the Herxheimer reaction.
Fruit can be re-introduced back into the diet FOUR WEEKS after the beginning of the Sanum remedies.
All capsules and tablets should be taken away from food and should not be taken together, as they clash. Follow this simple table below of how and when to take your Sanum remedies. These remedies are taken BEFORE or AWAY from food.
Open the capsules and pour the powder that they contain under the tongue and allow it to dissolve and absorb for a few minutes.
Prof. Enderlein’s Sanum remedies work by changing the harmful microorganisms in the body fluids into non- aggressive forms, probably by changing the pH and electrical conductivity. Harmful bacteria and toxins are broken down and excreted through natural processes. They also help to alleviate the dysbiosis and bring the internal mileau of the intestine back into balance.
Phase 5 – Balancing Body Chemistry
It is a commonly recognized and accepted fact that immune system efficiency is highly dependent on the proper biochemical balance in the body. This depends on proper and adequate nutrition to supply the body with all the required biochemical constituents (vitamins, minerals, enzymes, intrinsic factors).
Different people require different amounts and balances of nutrients for optimum health. The criteria for the determination of these differing nutritional requirements lies within the definition of one’s metabolic type, i.e., the genetically determined metabolic and nutritional parameters that define each person’s individuality on every level.
It is precisely because different people have different metabolic types, and therefore different needs for nutrition, that the allopathic, symptom- treatment approach in nutrition is baseless and so often ineffective.
The Blocking Factors of Recovery
Many time people who have Candidiasis don’t follow the Candida protocol precisely, consistently, and for a long enough period of time. Often when people feel better while they are on the Candida diet, they tend to go off it too quickly.
Often they don’t understand the need for its limitations, the importance of staying in tract, or the many substitutions that are available for problem foods or ingredients.
It has been found and research that it is beneficial to stay on the protocol until optimum health has been reached to the levels of treated.
Many people make the mistake of not rotate their foods on the protocol, and they repeat the same food more often. If they have a food family too often, they could easily develop intolerance to it, because the digestive system of the Candida sufferer is generally quite sensitive.
When people have Candida or CRC they usually have weakened immune systems. When the immune system is suppressed, it is prone to more infections and disease, making it impossible for a person to fully recover.
Depending on the severity of Candida overgrowth and the amount of the agents taken, the Candida can be killed off in vast numbers in a very short period of time. As they are killed, they release substances that are toxic to the body- mycotoxins. If the elimination organs such as the kidneys, liver, lymphatics, gut and skin cannot clear these mycotoxins quickly and then accumulate in the tissues, then a temporary toxic or allergic-type reaction can occur. The technical name for this experience is a Herxheimer reaction but it is more commonly referred to as “die off”.
Usually “die off” lasts only a few hours, though it can last several days. It can usually be controlled by reducing the dosage of the remedies used to kill the Candida, as well as taking drainage herbs and homoeopathics that your practitioner will advise you on.
Signs of Herxheimer reaction can be many and varied bur generally involve such discomfort as aching, bloating, dizziness, nausea. Exercise as well as insuring proper, daily bowel evacuation has been reported as being helpful in countering the adversities of die- off. Maintaining a high daily intake of pure water is also important to keep the channels of elimination open. Sometimes taking a teaspoon of baking soda (sodium bicarbonate) in a glass of water can help to quickly neutralize acidic reactions in the body that lead to inflammation and pain.
It may be possible to slow down these symptoms, many of which are caused by acetaldehyde, one of the main toxins produced by yeast. Taking molybdenum can break down this toxin into something far less harmful.
Adrenal gland dysfunction can create a complication to Candida recovery. This will affect the person’s ability to feel energized, cause the person to feel hot or cold temperatures more easily, possible sweat more than usual, heart palpitations, low sugar levels.
Lack of Hydrochloric acid (HCL)
HCL is produced in the stomach to aid in activating digestion of foods and protection of the intestinal flora.
One of the most common causes of HCL imbalances is past antibiotic use. Antibiotics destroy the beneficial bacteria that synthesize B vitamins necessary for HCL production in the stomach. Proper HCL levels in the stomach kill off many pathogens that otherwise would enter into the intestinal tract and potentially create problems.
HCL’s important functions include:
- Breaking down proteins into essential amino acids and nutrients
- Stimulating your pancreas and small intestines to produce the digestive enzymes and bile necessary to further breakdown the carbohydrates, proteins and fats
- Preventing disease by killing pathogenic bacteria and yeast normally present in foods.
- Low stomach acid leads to a cascade of digestive problems such as bloating, gas and constipation.
- Preventing the return of Candida
So if the patient suffers from hypochlorhydria or low production of hydrochloric acid from the stomach, then add a Betaine HCl + Pepsin supplement. In addition, if there is bloating, flatulence and a general discomfort of the gut, then one can add pancreatic enzymes too.
Natural Antibiotics During Candida Protocol
It is critical that anyone on the 3-month Candida protocol stock-up on NATURAL ANTIBIOTICS that they might require if they come down with a cold, flu, sore throat or any kind of infection while they are still on the Candida protocol.
These natural antibiotics have been tried and tested for many years and seem to work fine with most infections. However, it is very important to take these immediately when the first symptoms appear. If you leave the infection for a couple of days the microbes will spread quickly and it will be more difficult to shift it with the natural antibiotics.
This is why it is critical to have these natural antibiotics in your medical dispensary BEFORE beginning the Candida protocol – they have an expiry date of between 2 – 5 years, so you will no doubt use them during this time.
The dosages mentioned below are for adults. For maximal effectiveness it is good to use at least 4 of the natural antibiotics mentioned below, all in combination together.
These Natural antibiotics and herbal supplements include – link all the yellow to the site:
- Grapefruit seed extract (Citricidal): is a very effective anti-fungal, available in tablet form as well as liquid form which can be placed under nails with fungus. Take two tabs x 3 daily. For nails, one drop under each nail morning and evening.
- Oregano Oil – if one is citrus intolerant, then you can use Oregano oil gel caps instead – one gel cap x 3 times daily.
- Silver Liquid 50 ppm – you can take one teaspoon x 3 times daily.
- Vitamin C – take either 2 tabs (1000mg) x 3 daily, or ½ tsp x 3 times daily of the calcium ascorbate powder form.
- TRIFORM – a combination of a number of antibiotic herbs such as poke root, Echinacea, Berberine and more. Take 35 drops x 3 daily.
- Olive Leaf Extract – good to take one cap x 3 times daily if you know it is a viral infection.
If you regularly suffer from colds and flus, then it would be good to take about 1/3 tsp of vitamin C powder x 3 times daily – take this throughout the Candida Protocol. In addition, one can also take an immune-modulating product called EPICOR – one cap x 2 times daily.
Over the years Dr Georgiou has successfully treated in excess of 3,500 patients to date – here are just a few cases as examples:
CASE HISTORIES
CASE NO 1
Mrs. A, Age 44
Mrs. A’s presenting symptoms were somewhat unusual in that she continually complained that she frequently had the sense of a strong fishy odour in her nostrils over the last 7 years.
She remembers that this began when she had cleaned mould in her house with chlorine – the mould had appeared after a flood.
She also suffered from many allergies which included from a number of flowers, bananas and melon.
Her main symptoms apart from the annoying fishy odour was, constant intermittent coughing as well as a heavy pressure-type sensation in the chest and lungs. She had clear signs of nail fungus as well as frequent vaginal discharge.
She had consulted a number of medical doctors and dermatologists, but with no success. The dermatologist gave her antifungal cream for the nails. The condition remained as before.
She underwent bioresonance diagnosis using the VEGA system and was found to have a number of food intolerances too such as: wheat, lactose and milk products, bananas, caffeine, sugar, chicken, pork, nightshade family of vegetables (potatoes, tomatoes, peppers, and aubergines), olive oil and olives.
The VEGA test also showed that she was resonating with pathological, mycelial forms of Candida albicans, indicating that she was suffering from systemic Candidiasis – mixed moulds were also found during this testing protocol.
It was decided to help her body to detox and return back to an alkaline pH, as well as help eliminate inflammatory chemicals and other toxins. She followed an alkaline detoxification diet for 2 weeks based on alkaline foods such as fruit and vegetables.
Her energy levels after the detox had tremendously increased and she reported clarity of mind. She began the Da Vinci Candida Protocol for 3 months – see main text for details.
The smell of fish had decreased by 30% in intensity and the frequency to cough had also decreased by 40% within the first 3 weeks of the protocol treatment. After two months of treatment, the cough had improved 60%. Previously she would cough for one hour, now she coughs less than one minute. The smell of fish has improved by 70%.
After the completion of the Candida protocol (3 months), the Candida finally disappeared and the cough had improved by 100%. This was the first time that the cough had improved in the past 7 years. The smell of fish had also vanished as well as the nail fungus on her toes – this was also helped by adding grapefruit seed extract liquid – one drop per nail morning and evening. She was a very happy woman!
CASE NO 2
Mr. M, Age 45
Mr. M presented with a chronic cough that he had for the past 7-8 years, accompanied by whitish phlegm. He was diagnosed with H. Pylori for which the medical doctor prescribed antibiotics which were taken on and off for a period of 2 years. The coughing however persisted even though he had consulted many doctors, including ENT (otolaryngologists) and pneumonologists with no results. Before coughing began he lived in a mouldy apartment.
He underwent VEGA food intolerance testing that showed intolerance to a number of foods such as: wheat, soya, lactose and milk products, beans, caffeine, almonds and walnuts, pork, citrus (lemon, grapefruit, and oranges), olive oil and olives. He is a vegetarian but includes lactose and fish in his diet.
The VEGA testing also showed that he was suffering from systemic Candida albicans.
He followed an alkaline detoxification diet for 15 days based on fruit and vegetables. During the detox the cough had decreased by 50% in frequency and 70% decrease in intensity. The white phlegm had stopped completely.
Immediately after the detox he began the Da Vinci Candida protocol for 3 months. During the Candida protocol his energy levels had massively increased and he had incredible clarity of mind. After the Candida treatment his cough had completely vanished and the phlegm decreased to minimum.
CASE NO 3
Mrs. S, Age 49
Mrs. S complained that she had bronchial asthma and suffered from allergies. Medical doctors gave her cortisone sprays. She also suffers from obesity (147 kg) and whenever she tries to diet she suffers from hypoglycaemia.
Other health issues include atrial fibrillation (cardiac arrhythmia) and GERD- gastroesophageal reflux disease. She was taking Warfarin, an anticoagulant, to prevent blood clots from forming. She was also taking medication to control her arrhythmia.
She had also removed her thyroid nodules and was taking thyroxine daily.
It was recommended that she begin with a compromised alkaline detoxification diet lasting 1 month. This means that the body will be detoxing slower than the 15 days alkaline detox diet by leaving in protein foods the first two weeks. This procedure is recommended when there are chronic degenerative disease in order to prevent any possible adverse reactions caused by the elimination of inflammatory chemicals.
So, the first week of detox she was allowed to eat fish and pulses along with fruit and vegetables. The second week the fish was eliminated and only the pulses remained along with the fruit and vegetables. During the final two weeks she only ate fruit and vegetables.
During the detox her stomach digestion improved and she was feeling much better; oedema had also disappeared after some heavy urination initially, and she had lost noticeable inches around her waist – to her delight as weight had been blocked for a long time.
During bioresonance testing it was shown that she was intolerant to a number of foods such as: wheat, lactose and milk products, citrus (oranges, lemons, grapefruits), caffeine, sugar, hazelnut, walnuts, almonds, pork, chicken, and nightshade family of vegetables (potatoes, tomatoes, aubergines, peppers).
In addition, the Vega Bio-dermal testing also showed that she was suffering from systemic Candidiasis. She therefore began the Da Vinci Candida protocol for 3 months. During the Candida protocol she had lost a total of 12 kg, her asthmatic symptoms had gone completely, and she could now climb steps without wheezing and panting, being much quicker on her feet. As an added gift her chronic sinusitis had also completely cleared.
CASE NO. 4
Mrs J, 70 years old
We will be brief here – a 70 year old lady who had psoriasis most of her life was treated for systemic Candidiasis using the abovementioned protocol and within 90 days the psoriasis had cleared.
Before beginning the Candida protocol

3-months after completing the protocol

REFERENCES
Truss, CO. Metabolic abnormalities in patients with chronic Candidiasis – the acetaldehyde hypothesis, Journal of Orthomolecular Medicine, 13:63- 93, 1984
Gail Burton. Candida – The Silent Epidemic, Candida Causative factors, 4-9, 2003
Leon Chaitow N.D, D.O, Candida Albicans- Could yeast be your problem? How Candida gets out of hand. Chapter 3- Immune System Deficiency, 24-26, 1991
John Parks Trowbridge, M.D., and Morton Walker, D.P.M., The yeast syndrome- Antibiotics Encourage Yeast Overgrowth, 45-46, 1986
William G. Crook, M.D., Chronic Fatigue Syndrome and the yeast connection, Probiotics: 260,261, 1992
William G. Crook, M.D., The yeast connection – Candida questionnaire and score sheet – Diagnosis of a yeast-Related disorder, 29-33, Food allergies: 122, 1986
Hulda Regehr Clark, Ph.D., N.D., The Cure for all Diseases 1995
Crandall M. The pathogenetic significance of Intestinal Candida Colonization, 2004
Budtz- Jorgensen, E. Cellular immunity in acquired Candidiasis of the palate. Scand. J. Dent. Res. 81, 372, 1973
Hussein, H.S., and J.M. Brasel. Toxicity, metabolism, and impact of mycotoxins on humans and animals. Toxicology 167, 2001
Calderone, R.A., and R.L. Cihlar (e.d.). Fungal pathogenesis: principles and clinical applications. Marcel Dekker, Inc., New York, N.Y, 2002
Trowbridge JP and Walker M. The yeast Syndrome Bantam Books, New York, N.Y, 1986
Truss C: The missing Diagnosis Birmingham Alabama (The Author), 1983
Crook WG: The yeast connection, A medical Breakthrough 2nd Addition Professional Books, Jackson, TN, 1984
Michael T. Murray, N.D., Chronic Candidiasis, Dietary factors, sugar and the yeast syndrome: 43,44, 1997
Dr Georgiou has been an active clinician for 30 years, and Director Founder of the Da Vinci Holistic Health Centre and the Da Vinci College of Holistic Medicine in Larnaca, Cyprus